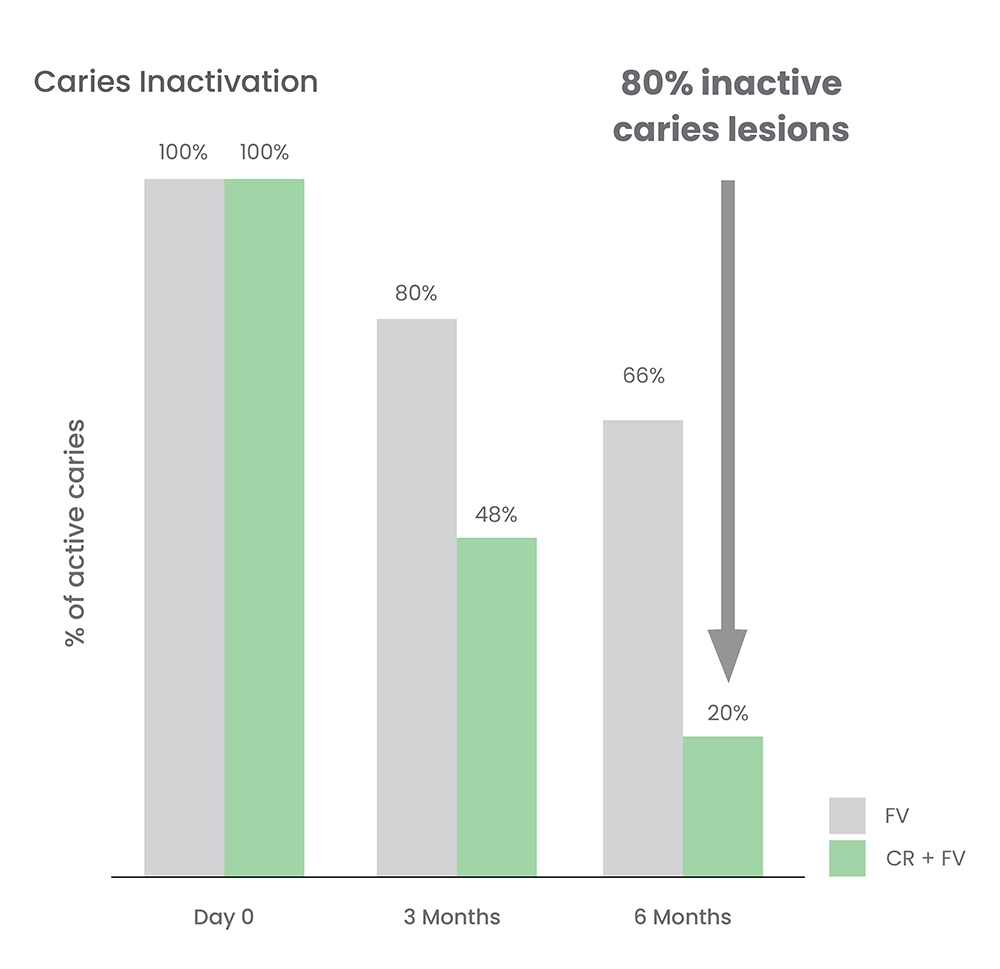
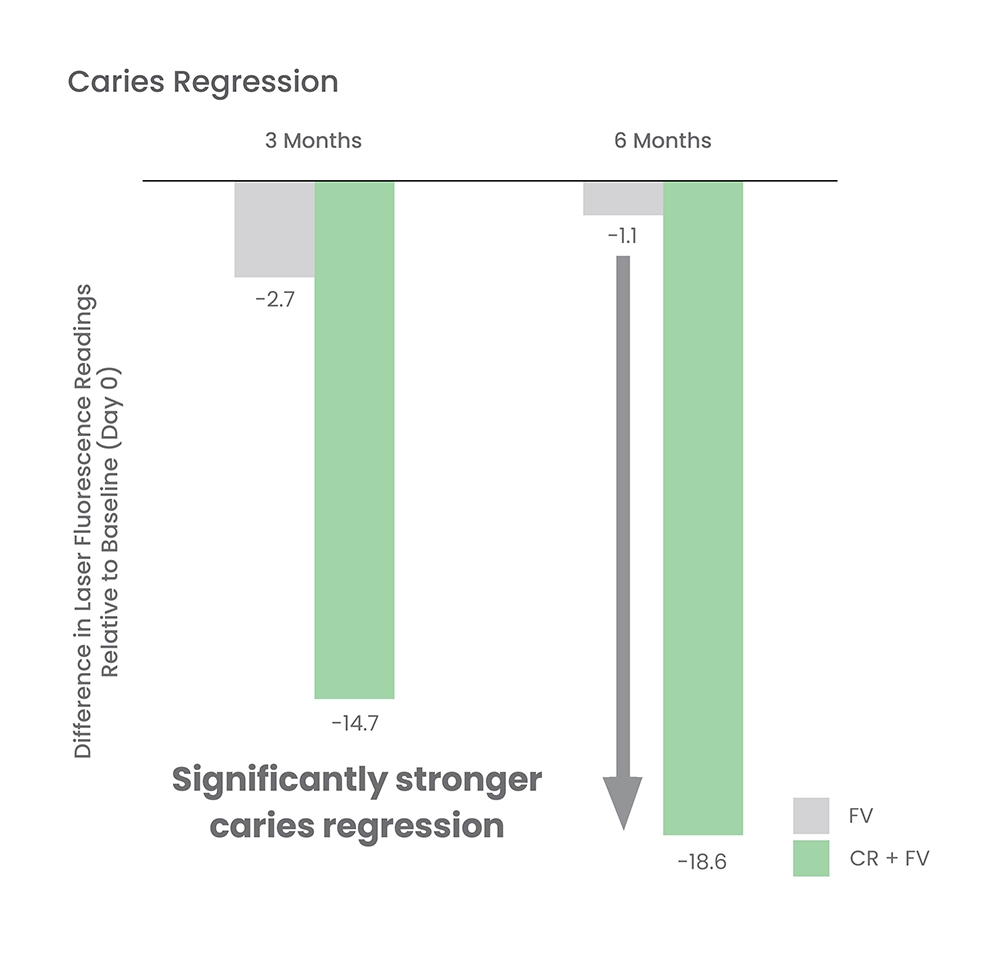
No. CurodontTM Repair can be used in conjunction with other remineralising agents, such as fluoride varnish, to optimize enamel regeneration and mineralization. In fact, the concurrent use of CurodontTM Repair and fluoride varnish has been successfully used to produce greater inactivation of caries compared to fluoride varnish alone.*
However, all treatments should be carried out only after an interval of at least 5 minutes after the application of CurodontTM Repair and not before.
*Alkilzy M, Tarabaih A, Santamaria RM, Splieth CH. Self-assembling Peptide P11-4 and Fluoride for Regenerating Enamel. J Dent Res. 2018 Feb;97(2):148-154.
Doberdoli D et al. Randomized Clinical Trial investigating Self-Assembling Peptide P11-4 for Treatment of Early Occlusal Caries. Sci Rep 2020;10:4195.